Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Spinal and Epidural Anesthesia Yuri Krylov Rabin Medical Center – Beilinson Campus

2
Procedures To Be Done Spinal Anesthesia: –Lower extremities surgery –Hip surgery –Lower abdominal surgery –Proctology –TUR –Vaginal/cervical surgery Epidural Anesthesia –Labor and delivery –Same as under spinal –Thoracic surgery –Cardiac surgery –Postoperative pain relief –Chronic pain management

3
Anatomy Vertebrae Ligaments Epidural Space Meninges –Dura Mater –Arachnoid Mater –Pia Mater Spinal Cord

4
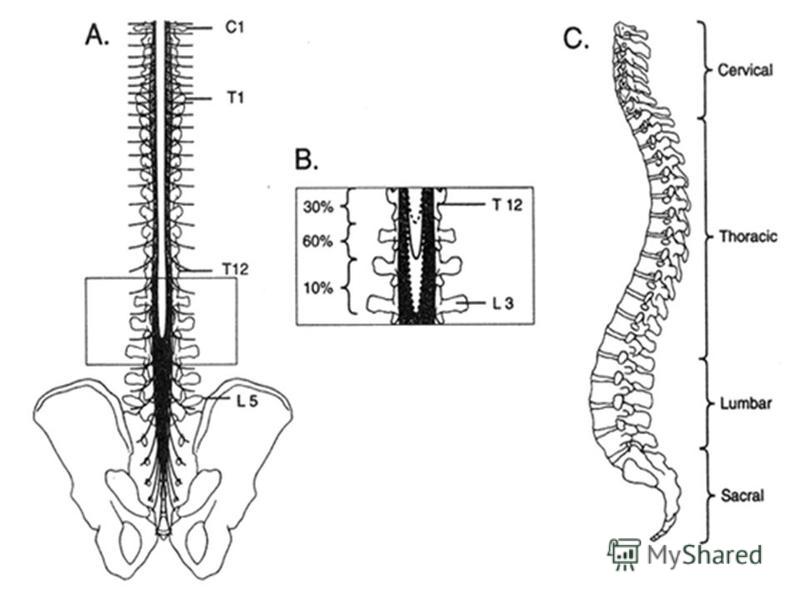
Vertebrae 33 vertebrae: –7 cervical –12 thoracic –5 lumbar –5 sacral (fused) –4 coccygeal (fused) C7 – the first prominent spinous process L5 – a line between iliac crests
 –4 coccygeal (fused) C7 – the first prominent spinous process L5 – a line between iliac crests")
5
Ligaments 1.Supraspinous Ligament (from Sacrum to T7) 2.Ligamentum Muchae (T7 – base of skull) 3.Interspinous Ligament (spinous processes) 4.Ligamentum Flavum 5.Anterior and Posterior Longitudinal Ligaments
 2.Ligamentum Muchae (T7 – base of skull) 3.Interspinous Ligament (spinous processes) 4.Ligamentum Flavum 5.Anterior and Posterior Longitudinal Ligaments")
6
Epidural Space Lies between the spinal meninges and the sides of the vertebral canal The most ubiquitous material is fat, which is located in the posterior and lateral epidural space Plays a role in the pharmacokinetics of local anesthetics

7
Meninges Dura Mater –outermost and thickest meningeal tissue –begins at the foramen magnum –caudally ends at approximately S2 Arachnoid Mater –delicate, avascular membrane –the subarachnoid space lies between the arachnoid mater and the pia mater and contains CSF Pia Mater –adherent to the spinal cord

9
Spinal Cord In the adult, the caudal tip of the spinal cord typically lies at L1 In 30% of people the spinal cord ends at T12 In 10% may extend to L3 Flexion of the vertebral column causes the tip of the spinal cord to move slightly cephalad

11
Spinal Cord 31 pairs of spinal nerves: –anterior motor root –posterior sensory root Cord Segment – the portion of the spinal cord that gives rise to all of the rootlets of a single spinal nerve Dermatome – the skin area innervated by a given spinal nerve

13
Physiologic Action Sensor block –Lack of pain and temperature sensation –Presence of tactile sensation Motor block –Weakness or immobility of extremities –Weakness of respiratory muscles* Sympathetic block –Hypotension –Bradycardia*

14
Agents To Be Used Local anesthetics: –Amides –Esters Opiates (improves quality of sensor block) α-2 adrenergic agonists (synergy with LA) Epinephrine ( systemic absorption of LA) Sodium bicarbonate (alkalinization)
 α-2 adrenergic agonists (synergy with LA) Epinephrine ( systemic absorption of LA) Sodium bicarbonate (alkalinization)")
15
Technique Appropriate monitors: –5 leads ECG –SpO 2 –NIBP at least every 5 or IBP Equipment for airway management and resuscitation is immediately available Sterile conditions At least one assistant

17
Patients Position Lateral decubitus position –Most often used Prone jackknife –When its the position to be used for surgery Sitting positions –Obese patients –Saddle block

18
Spinal Anesthesia

19
Epidural Anesthesia

20
Contraindications Absolute –Patient Refusal Relative –Hypovolemia / Shock –Increased ICP –Coagulopathy / Thrombocytopenia –Sepsis / Infection at the puncture site –Preexisting neurologic disease

21
Anticoagulants and Antiaggregants Stop beforeReinstituteLab TestReversal Coumadin 4-5 days24 hPT/INRFFP x 4 Heparin sc 8 h1 hPTT, ACTProtamine Heparin iv 4 h1 hPTT, ACTProtamine LMWH h2 hAnti-Xa*Time NSAIDs Not risk

22
Complications Backache Postdural Puncture Headache (PDPH) Epidural abscess/meningitis Systemic Toxicity Total Spinal Neurologic Injury Spinal Hematoma Accidental Intravascular Injection
 Epidural abscess/meningitis Systemic Toxicity Total Spinal Neurologic Injury Spinal Hematoma Accidental Intravascular Injection")
23
Backache The most common complication Incidence: –11% after spinal block –30% after epidural block Etiology: –Needle trauma –Local anesthetic irritation –Ligamentous strain The most common reason to refuse future block

24
Postdural Puncture Headache (PDPH) Incidence: –Less 1% after spinal block –Up to 50% after accidental dural puncture –Decrease with age The Pain: –Fronto-occipital –Absent in supine –Head elevation leads to severe headache
 Incidence: –Less 1% after spinal block –Up to 50% after accidental dural puncture –Decrease with age The Pain: –Fronto-occipital –Absent in supine –Head elevation leads to severe headache")
25
Postdural Puncture Headache (PDPH) Usually resolves spontaneously (days - week) Conservative Treatment: –Bed rest –Analgesics –Fluids –Caffeine Epidural Blood Patch –20 ml autologous blood –85-95% efficiency within 1-24 hours
 Usually resolves spontaneously (days - week) Conservative Treatment: –Bed rest –Analgesics –Fluids –Caffeine Epidural Blood Patch –20 ml autologous blood –85-95% efficiency within 1-24 hours")
26
Neurologic Injury 0.03% - 0.1% of all neuraxial blocks Paresthesias and limited motor weakness are most common Mechanism Of Injury –Direct needle trauma –Spinal cord ischemia –Injection of neurotoxic drugs –Epidural hematoma Transient Neurologic Symptoms (TNS) –Pain or dysesthesia in the legs after spinal with Lidocaine –Usually resolves spontaneously within 72 hours

27
Spinal and Epidural Hematoma <1 in 150,000 patients Increased risk: –Anticoagulants –Antiplatelets drugs Numbness or lower extremity weakness Early detection is critical (MRI) Golden Hour – 8 hours since the symptoms appeared
 Golden Hour – 8 hours since the symptoms appeared")
28
Epidural Hematoma

29
Spinal or Epidural ? Spinal: –Takes less time to perform –Produces more rapid onset –Better-quality sensorimotor block –Associated with less pain during surgery Epidural –Lower risk of PDPH –Less hypotension if epinephrine is not added to the local anesthetic –Ability to prolong or extend the block using an indwelling catheter –The option of provide postoperative analgesia

Еще похожие презентации в нашем архиве:








 A neurosurgeon is a surgeon who specializes in operating on the brain, head, neck, and spinal cord.")













. 2001. NOAA Diving Manual - Diving for Science and Technology, Fourth Edition. Best.")