Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Students Scientific Society, I.M. Sechenov Moscow Medical Academy Beh Jien Wey Medical faculty, English Medium, Group 8 Scientific supervisor : Prof. E. A. Kogan

2
Nephroblastoma (Wilms tumor) Definition : malignant embryonal neoplasm derived from nephrogenic blastemal cells that both replicates the histology of developing kidneys and often show divergent patterns of differentiation
 Definition : malignant embryonal neoplasm derived from nephrogenic blastemal cells that both replicates the histology of developing kidneys and often show divergent patterns of differentiation")
3
Epidemiology Affects approximately 1 in every 8000 children worldwide No prominent sex predilection Equal frequency in both kidneys Average age at diagnosis Males : 37 months Females :48 months 98% of cases occur in individuals under 10 years old No environmental factors involved in development General risk is higher in African-Americans; lower in Asians

4
STAGES OF NEPHROBLASTOMA Stage I Renal sinus soft tissue may be minimally infiltrated, without any involvement of the sinus vessels. The tumor may protrude into the pelvic system without infiltrating the wall of the ureter. Intrarenal vessels may be involved.

5
STAGES OF NEPHROBLASTOMA Stage II Tumor penetration of renal capsule or infiltration of vessels within the renal sinus (including the intrarenal extension of the sinus). Tumor infiltrates adjacent organs or vena cava but is completely resected.
. Tumor infiltrates adjacent organs or vena cava but is completely resected.")
6
STAGES OF NEPHROBLASTOMA Stage III Involvement of specimen margins grossly or microscopically Tumor in abdominal lymph nodes; Diffuse peritoneal contamination by direct tumor growth, tumor implants, or spillage into peritoneum before or during surgery; Residual tumor in abdomen

7
STAGES OF NEPHROBLASTOMA Stage IV Hematogenous metastases or lymph node metastasis outside the abdominopelvic region. Stage V Bilateral renal involvement at diagnosis Prognosis depends on presence of anaplasia

8
CLINICAL FEATURES Usually comes into attention when there is an abdominal mass in children Other presentations include : Abdominal pain Hematuria Acute abdominal crisis secondary to traumatic rupture Anemia Hypertension due to overproduction of renin Polycythemia due to tumoral erythropoietin production

9
CLINICAL TREATMENT Majority are treated using protocols from International Society of Paediatric Oncology (SIOP) or the Childrens Oncology Group (COG). SIOP protocol : advocate preoperative therapy followed by surgical removal. allows for tumour shrinkage prior to resection, yielding a greater frequency and ease of complete resectability
 or the Childrens Oncology Group (COG). SIOP protocol : advocate preoperative therapy followed by surgical removal. allows for tumour shri")
10
COG protocol Advocated primary resection of tumours, followed by therapy that is determined by stage and classification into "favourable and "unfavourable" histology categories. This allows for greater diagnostic confidence and greater ability to stratify patients according to pathologic and biologic parameters.

13
MACROSCOPY Most nephroblastomas are unicentric But, multicentric variants are also present: Unilateral in 7% of cases Bilateral in 5% of cases Nephroblastomas are solitary rounded masses sharply demarcated from the adjacent renal parenchyma by a peritumoural fibrous pseudocapsule Color : grey or tan Consistence : soft [may appear firm and whorled if a large fraction of the lesion is composed of mature stromal elements]

16
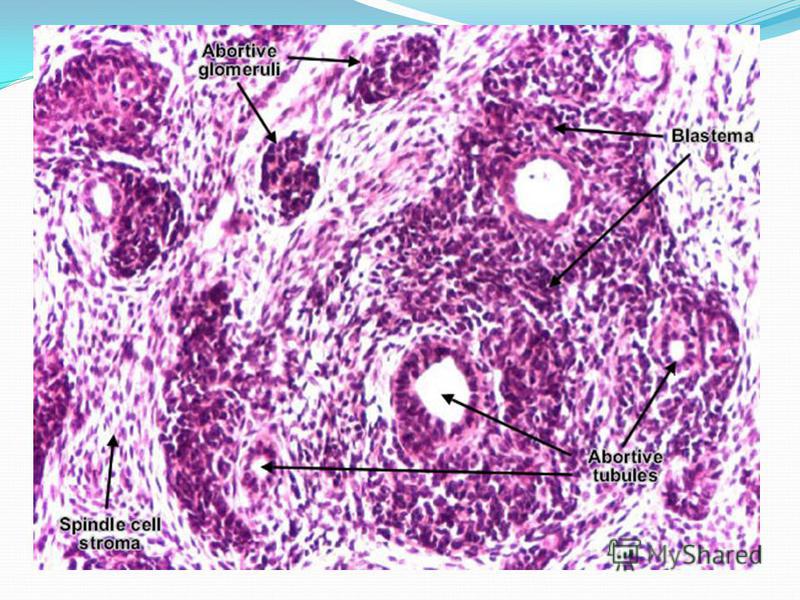
HISTOPATHOLOGY Nephroblastoma contains : undifferentiated blastemal cells cells differentiating to various degrees and in different proportions toward epithelial and stromal lineages Triphasic patterns are the most characteristic, but biphasic and monophasic lesions are often observed Non renal elements, such as skeletal muscle and cartilage occur

17
Blastemal cells small, closely packed, mitotically active rounded or oval cells with scant cytoplasm overlapping nuclei containing evenly distributed, slightly coarse chromatin, and small nucleoli 1. Diffused blastemal pattern lack of cellular cohesiveness and an aggressive pattern of invasion into adjacent connective tissues and vessels 2. Nodular & serpentine patterns round or undulating, sharply defined cords or nests of blastemal cells set in a loose fibromyxoid stroma

18
Epithelial cells Present in most nephroblastomas Manifested by primitive rosette-like structures barely recognizable as early tubular forms Heterologous epithelial differentiation may occur, the most common elements – mucinous and squamous epithelium

19
Stromal cells A variety of patterns occur may cause diagnostic difficulty when blastemal and epithelial differentiation, are absent. Smooth muscle, skeletal muscle and fibroblastic differentiation may be present Other types of heterologous stromal differentiation include : Adipose tissue Cartilage Bone Ganglion and neuroglial cells

20
NEPHROBLASTOMA Undifferentiated blastemal cells Differentiated cells Epithelial Stromal

25
TYPES OF WILMS TUMOR Bilateral (<10%) Associated with gross congenital syndrome – WAGR (Wilms tumor, Arinidia, Genitourinary malformation, mental Retardation) (30%) Familial (rare, <1%)
 Associated with gross congenital syndrome – WAGR (Wilms tumor, Arinidia, Genitourinary malformation, mental Retardation) (30%) Familial (rare, <1%)")
27
KNUDSONS TWO-HIT MODEL A genetic model of tumor-suppressor genes States that individuals with a family history of cancer carry a germline mutation in one allele of a tumor-suppressor gene, and therefore require only one additional 'hit' to cause somatic homozygosity by inactivating the second allele Individuals with no such predisposition require two independent genetic events (2 hits on alleles)

28
GENETICS OF TUMOR Inherited mutations at WT-1 Familial-predisposition loci FWT-1 / WT-4 (Familial Wilms Tumor 1) At 17q12-q21 FWT-2 At 19q13.4
 At 17q12-q21 FWT-2 At 19q13.4")
30
GENETICS OF TUMOR WAGR syndrome : Consistent deletion of chromosome 11p13 in somatic cells involving WT-1 gene WT-1 encodes a zinc finger transcription factor that plays a major role in renal and gonadal development Denys-Drash syndrome : Mesangial sclerosis, pseudohermaphroditism Constitutional inactivating point mutations in one copy of WT1 Loss of remaining normal WT-1 in tumor

31
METASTASIS Generally restricted pattern of metastasis Common sites : Regional lymph nodes Lung Liver

32
Metastasis in Stage IV with favorable histology

33
PROGNOSIS Most nephroblastomas are of low stage and favorable histology, thus GOOD prognosis Tumors that demonstrate extensive blastemal cells following therapy lead to POOR prognosis, survival rate is LOW (blastemal chemoresistant tumor – treated like anaplastic tumor) Current survival rate : 85-90%

34
- the end - Thank you

Еще похожие презентации в нашем архиве:











 ~ 1% of pts undergoing.")














. Family How could you describe the word family? First of all family means a close unit of parents and their.")