Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Staphylococci Facultative, non-sporulating, non-motile, Gram positive cocci Cell Division 3 planes –Daughter cells dont fully separate form clusters Greek nouns –Staphyle – a bunch of grapes –Coccus – grain or berry

2
Staphylococci 27 species Three Important Species Staphylococcus aureus –Important human pathogen Staphylococcus epidermidis –Normal skin flora, disease under special circumstances Staphylococcus saprophyticus –UTIs in young females

3
S. aureus S. epidermidis S. saprophyticus Catalasepositivepositivepositive Coagulase positive negativenegative Novobiocin negativenegativepositive Resistance

4
STAPHYLOCOCCI - Cell Wall 1)Peptidoglycan – main component of the cell wall Hydrated, semi-rigid polymer of two sugar derivatives: N-Acteylglucosamine & N-Acetylmuramic acid 90% of cell wall may contain peptidoglycan Less in Gram negative organism
Peptidoglycan – main component of the cell wall Hydrated, semi-rigid polymer of two sugar derivatives: N-Acteylglucosamine & N-Acetylmuramic acid 90% of cell wall may contain peptidoglycan Less in Gram negative organism")
5
STAPHYLOCOCCI - Cell Wall 2) Teichoic Acid Polymer of glycerol or ribitol joined by phosphate groups Covalently linked to muramic acid of peptidoglycan Links various layers of the peptidoglycan mesh together. 2 classes of teichoic acids Lipoteichoic acid –Embedded in the peptidoglycan layer –Linked to the cytoplasmic membrane Wall teichoic acid –Linked to only the peptidoglycan layer Teichoic acid is responsible for the antigenic determinant of the organism
 Teichoic Acid Polymer of glycerol or ribitol joined by phosphate groups Covalently linked to muramic acid of peptidoglycan Links various layers of the peptidoglycan mesh together. 2 classes of teichoic acids Lipoteichoic")
6
STAPHYLOCOCCI - Cell Wall 3) Protein A –Bind the Fc component of antibodies 4) Coagulase –Bound and soluble forms –Activates the coagulation cascade Fibrin meshwork abscess formation 5) Capsule –Variable
 Protein A –Bind the Fc component of antibodies 4) Coagulase –Bound and soluble forms –Activates the coagulation cascade Fibrin meshwork abscess formation 5) Capsule –Variable")
7
S. aureus - Epidemiology Reservoir – Humans Asymptomatic Carriage Sites: –Nares –Rectum –Perineum –Pharynx Skin Colonization - Brief, Repeated Transmission - Person to Person

8
S. aureus Carriage Rates PopulationCarriage Rate (%) General Population 25 Hemodialysis75 Diabetic on insulin50 Patients receiving 50 allergy shots Intravenous Drug Users40
 General Population 25 Hemodialysis75 Diabetic on insulin50 Patients receiving 50 allergy shots Intravenous Drug Users40")
9
Staphylococcal Infections - Risk Factors Skin Disease – Increased colonization Trauma –Expose binding sites Viral Respiratory Tract Infection (Influenza) –Expose binding sites –Decreased clearance Foreign Body Liver disease Neoplasia Diabetes Renal Failure Leukocyte & Immunoglobulin Defects Elevated Serum IgE Levels Narcotics Addiction Broad Spectrum Antibiotic Therapy In general Healthy people dont get serious Staph infections
 –Expose binding sites –Decreased clearance Foreign Body Liver disease Neoplasia Diabetes Renal F")
10
Patterns of Disease - S. aureus 1)Invasion with Tissue Destruction 2) Toxin Mediated –Toxic Shock Syndrome –Scalded Skin Syndrome –Staphylococcal Food Poisoning
Invasion with Tissue Destruction 2) Toxin Mediated –Toxic Shock Syndrome –Scalded Skin Syndrome –Staphylococcal Food Poisoning")
11
S. aureus - Invasive Infections A Two Step Process: 1.Binding (adherence) to host tissues 2.Invasion
 to host tissues 2.Invasion")
12
Staphylococcal Virulence Factors - Adherence 1) Nasal Mucosa –Teichoic Acid 2) Traumatized Skin and Foreign Surfaces Breech in normal barrier of mucosa or skin Unmasked host proteins that S. aureus has specific receptors Fibronectin Fibrinogen Laminin Type IV collagen 3) Endothelial Cell S. aureus has a unique affinity for the vascular tree Attach to Fibronectin, Laminin and Endothelium Itself
 Nasal Mucosa –Teichoic Acid 2) Traumatized Skin and Foreign Surfaces Breech in normal barrier of mucosa or skin Unmasked host proteins that S. aureus has specific receptors Fibronectin Fibrinogen Lamini")
13
Staphylococcal Virulence Factors - Invasion A. Tissue Degrading Enzymes 1) Hyaluronidase Hydrolyzes hyaluronic acid in connective tissue matrix 2) Lipase Break down lipids in matrix 3) DNase 4) Hemolysins and Leukocidins Family of membrane damaging toxins Dissolve RBCs, WBCs and tissue cells 5) Coagulase Causes plasma to clot –Promotes abscess formation (wall) –Fibrin deposition around bacteria may protect from phagocytosis
 Hyaluronidase Hydrolyzes hyaluronic acid in connective tissue matrix 2) Lipase Break down lipids in matrix 3) DNase 4) Hemolysins and Leukocidins Family of membrane damaging t")
14
Staphylococcal Virulence Factors - Invasion B. Anti-Phagocytic Factors 1) Catalase Made by all Staph (not Streptococcus) Leukocytes use oxidative mechanism to kill bacteria –Inactivates Hydrogen Peroxide H 2 O + O 2 2) Protein A Binds the Fc component of IgG Inhibits opsonization by antibody 3) Capsule Stearic Hindrance Variable
 Catalase Made by all Staph (not Streptococcus) Leukocytes use oxidative mechanism to kill bacteria –Inactivates Hydrogen Peroxide H 2 O + O 2 2) Protein A Binds the Fc componen")
15
Anterior Nares Skin Trauma Localized Colonization Infection BacteremiaMetastatic Foci Lungs Endocarditis Liver/Spleen CNS Kidneys

17
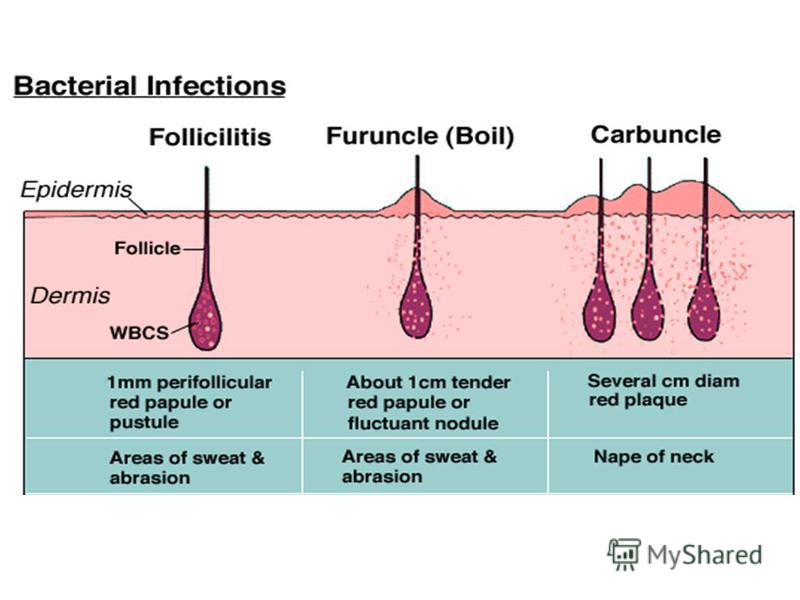
Furuncle Often starts as infection of hair follicle Folliculitis Firm, tender red nodule Painful Fluctuant with time Drain spontaneously

18
Carbuncle Larger than furuncle Extends into subcutaneous fat Interconnected Firm, inelastic skin

20
Impetigo Superficial infection of skin Usually –S. aureus –Streptococcus pyogenes Children Hot Weather Minor Trauma Initially vesicles

21
Impetigo Later: Crusted with yellow dark brown material

22
Erysipelas Strep pyogenes or S. aureus Sharp, raised borders

23
Cellulitis Acute, spreading Infection Involves both skin and subcutaneous tissues Prior trauma to skin Warm and erethematous

24
Mitral Valve Endocarditis

25
Endocardits

26
Patterns of Disease - S. aureus 1)Invasion with Tissue Destruction 2) Toxin Mediated –Toxic Shock Syndrome –Scalded Skin Syndrome –Staphylococcal Food Poisoning
Invasion with Tissue Destruction 2) Toxin Mediated –Toxic Shock Syndrome –Scalded Skin Syndrome –Staphylococcal Food Poisoning")
27
TOXIC SHOCK SYNDROME Todd and coworkers reported a group of children: Acute Febrile Illness Subsequent Development of Hypotension and Shock. Noted association with S. aureus phage group I Named the illness "Toxic Shock Syndrome Illness had been identified in 941 patients in the USA More than 3,300 cases have been reported 95% in women 90% occurred during menstruation in women who were using tampons cases of TSS reported

28
Toxic Shock Syndrome - Epidemiology 1. Menstrual Colonization of the Vagina and Cervix with TSST-1 producing strains of S. aureus –Tampon Associated Risk proportional to the absorbancy of Tampon –Not tampon associated 2. Non-menstrual Post-surgical Influenza associated Contraceptive device associated –Diaphragm –Sponge Postpartum

29
Pyrogenic Toxin Family of Proteins secreted by –S. aureus –Strep pyogenes Share biologic properties and Amino Acid Sequences –Molecular wgt: 20,000 30,000 daltons Include –TSST-1 –Staphylococcal Enterotoxins A, B,C –Pyrogenic Exotoxin A & B –Streptococcal Scarlet Fever Toxins A, B,C

30
TSST – A Superantigen Able to activate large number of Tcells –Up to 20% at one time Massive Cytokine Release Interacts directly with invariable region of Class II MHC molecule Activated T Cells Release –IL-1: pyrogen, muscle proteolysis –IL-2 –TNF : inhibit PMN function –IFN-

31
Physicochemical Factors that Promote TSST-1 Production 1) Protein (or amino acid) containing environment 2) Temperature 37 o C - 40 o C 3) Ph range ) Presence of Oxygen
 Protein (or amino acid) containing environment 2) Temperature 37 o C - 40 o C 3) Ph range 6.5 - 8 4) Presence of Oxygen")
32
Toxic Shock Syndrome - Clinical Manifestations 1. High Fever (>39.9 o C) 2. Scarlatiniform Eruption 3. Hypotension and Shock 4. Desquamation during convalescence
 2. Scarlatiniform Eruption 3. Hypotension and Shock 4. Desquamation during convalescence")
33
Manifestations of Specific Organ Involvement Mucous Membranes: hyperemia Gastrointestinal Tract: vomiting and diarrhea Muscle: severe myalgias Central Nervous System: disorientation Kidney: azotemia, pyuria urinary tract infection Liver: elevation of serum bilirubin and SGOT Blood: Thrombocytopenia

34
Toxic Shock Syndrome - Diagnosis Isolation of toxin producing S. aureus from a patient with a compatible clinical illness.

35
Toxic Shock Syndrome - Treatment 1) Treatment of Hypotension and Shock –Vigorous Fluid Replacement 2) Attention to the Site of S. aureus Colonization –Removal of Tampons –Drainage of Staphylococcal Abscess 3) Anti-Staphylococcal Antibiotic Therapy
 Treatment of Hypotension and Shock –Vigorous Fluid Replacement 2) Attention to the Site of S. aureus Colonization –Removal of Tampons –Drainage of Staphylococcal Abscess 3) Anti-Staphylococcal Antibiotic Therapy")
36
STAPHYLOCOCCAL SCALDED SKIN SYNDROME A Disease of Infants –Localized Infection with Diffuse Skin Rash S. aureus (Phage group II) recovered from: –Nose –Pustules –Eye –Umbilicus Exfoliative Toxin –Two Serologically and Biologically Distinct Proteins Exfoliatin A Exfoliatin B –Inter-Epithelial Splitting of Stratum Granulosum Layer
 recovered from: –Nose –Pustules –Eye –Umbilicus Exfoliative Toxin –Two Serologically and Biologically Distinct Proteins E")
37
Staphylococcal Scalded Skin Syndrome - Clinical Features Starts Abruptly –Perioral erythema –Sunburn like, tender rash spreads over entire body Bullae Appear Rapidly –Nikolsky sign –Flaccid bullae slough off Denuded areas Exfoliated Areas Eventually Dry –Flaky desquamation lasting 3-5 days Within 10 days After Onset Complete Recovery –New epidermis has replaced the denuded areas

38
Staphylococcal Food Poisoning 20% of Outbreaks of Acute Food Poisoning Toxigenic Strain of S. aureus growing in contaminated food –Produces Enterotoxin B (Heat Stable) Person to Person Transmission –Responsible organism usually isolated from person involved meal preparation Commonly implicated foods –Custard filled bakery good –Canned food –Potato salad –Ice cream Food appears normal in appearance, odor and taste
 Person to Person Transmission –Responsible organism usually isolated from person i")
39
Staphylococcal Food Poisoning - Clinical Features Incubation period 2-6 hours Enterotoxin stimulates intestinal peristalsis and CNS –Abrupt onset: Salivation Nausea and vomiting Abdominal cramps Watery diarrhea Afebrile Self limited, symptoms disappear in 8 hours

40
S. aureus Treatment 1941 – Penicillin available 1945 – Penicillin resistance reported –Plasmid mediated –2 o to beta-lactamase (penicillinase) Semi-synthetic pencillins produced –Methacillin, oxacillin, nafcillin 1961 Methacillin resistant S. aureus (MRSA) reported –Resistant to all beta-lactam antibiotics
 1960-64 Semi-synthetic pencillins produced –Methacillin, oxacillin, nafcillin 1961 Methacillin resistant S.")
41
Methacillin Resistant S. aureus (MRSA) 2 Penicillin binding proteins (PBPs) normally have enzymatic activity responsible for cross linking peptidoglycan wall MRSA have acquired a chromosomal gene MecA code for alternate PBP (PBP 2a) –Low affinity for beta lactam –Enzymatically active generate peptidoglycan Treatment Vancomycin (glycopeptide AB)
 2 Penicillin binding proteins (PBPs) normally have enzymatic activity responsible for cross linking peptidoglycan wall MRSA have acquired a chromosomal gene MecA code for alternate PBP (PBP 2a) –Low affinity for")
42
Glycopeptide Resistant S. aureus First reported in 1997 Increased production of cell wall precursors including PBP2a –Soak up antibiotic in thickened cell wall

43
Staphylococcus epidermidis Normal Flora –Virtually all humans carry S. epidermidis on the skin and in and around body orifices Hospital Acquired Infection –Contamination by S. epidermidis carried by the patient most important event in infections associated with foreign bodies

44
S. epidermidis - Virulence Factors Production of an exo-polysaccharide ("slime") Promotes adherence to plastic surfaces Increases resistance to phagocytosis Increases resistance to antimicrobial therapy
 Promotes adherence to plastic surfaces Increases resistance to phagocytosis Increases resistance to antimicrobial therapy")
45
S. epidermidis - Patterns of Infection Nosocomial Bacteremia -most common cause Endocarditis A. Native Valve –Uncommon- 5% of cases B. Prosthetic Valve –Single most common cause (40% of cases) –Probably caused by inoculation at the time of surgery –Indolent course Intravenous Catheters -Single most common cause (50-75% of cases) Cerebrospinal Fluid Shunts Peritoneal Dialysis Catheter Vascular Grafts Prosthetic Joints
 –Probably caused by inoculation at the time of surgery –I")
46
Foreign Body - Mechanisms of Staphylococcal Persistence 1) Fibronectin and Fibrinogen Coating –Firm Anchor for Staphylococci 2) Glycocalyx Production –Protects Bacteria 3) Dysfunctional Phagocyte Population –Incapable of Killing Bacteria
 Fibronectin and Fibrinogen Coating –Firm Anchor for Staphylococci 2) Glycocalyx Production –Protects Bacteria 3) Dysfunctional Phagocyte Population –Incapable of Killing Bacteria")
47
S. epidermidis Infection - Treatment 1. Antimicrobial Therapy Usually resistant to multiple antibiotics –Beta lactams –Erythromycin, Clindamycin, Tetracycline Require therapy with Vancomycin 2. Removal of Foreign Body

48
Staphylococcus saprophyticus Colonizes the genitourinary mucosa of some young women Causes both upper and lower urinary tract disease –95% of cases are in females years old –Responsible for 20 of the UTI's in this age group Second only to E. coli Pathogen of young, sexually active females –70% sexual intercourse within 24 hours preceding onset of symptoms

Еще похожие презентации в нашем архиве:





 Ventilator-associated pneumonia (VAP) is defined as nosocomial pneumonia in a patient on mechanical ventilatory support.")



 Invades the helper T cells (CD4 cells) in the body of the host.")