Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Extrapyramidal system and Cerebellum

2
Extrapyramidal system consists of: cortical areas 4, 6, 8 the basal ganglia: n. caudatus, n.lenticularis (putamen, globus palidus) the nuclei of brain stem (black substance, red nucleus, vestibular nuclei, reticular nuclei, nucleus of Darkshevych, Lues body, lower olives) spinal cord: -motor neurons and -small motor neurons, which are located in anterior horns of the spinal cord
 the nuclei of brain stem (black substance, red nucleus, vestibular nuclei, reticular nuclei, nucleus of Darkshevych, Lu")
3
Two parts of Extrapyramidal system: Pallidum globus palidus black substance red nuclei vestibular nuclei nucleus of Darkshevych lower olives Lues body Pallidum is phylogenetically older then striatum. Thats why in newborn babies pallidum dominates

4
Two parts of Extrapyramidal system: Striatum cortical areas 4,6,8 n. Caudatus Putamen Only at the age of 4 – 5 months old striatum starts to influence on motor functions

6
Connections of Extrapyramidal system: Pallidum and striatum are closely connected with each other by means of such pathways: nigrostriatal (dopaminergic) – black substance – nucleus caudated – it inhibits the neurons of striatum strionigral (GABA-ergic)- nucleus caudated (GABA) – black substance – it controls production of dopamine.
 – black substance – nucleus caudated – it inhibits the neurons of striatum strionigral (GABA-erg")
7
The afferent pathways of Extrapyramidal system : T – EPNS – T T – cortex – EPNS – T T – cortex - pons – cerebellum – thalamus The efferent pathways of Extrapyramidal system: Tr. olivospinalis Tr. rubrospinalis Tr. vestibulospinalis Tr. tectospinalis Tr. reticulospinalis

8
Functions of Extrapyramidal system It prepares muscles to smooth economical movements It determines the posture It makes automatical involuntary regulation of active conscious movements It provides automatical stereotyped movements and reflector protective movements It provides motor manifestation of emotions

9
Extrapyramidal systems lesion: Parkinsons syndrome (lesion of pallidum) Syndrome of involuntary movements (lesion of striatum)
 Syndrome of involuntary movements (lesion of striatum)")
10
Parkinsons disease In 1817 – James Parkinson described the major manifestation of this syndrome In 1874 – this disease was called after James Parkinson – Parkinsons disease In 1920 – Tretiakov noticed that the greater cell loss in substantia nigra, the lower concentration of dopamine is in striatum and more severe the degree of clinical Parkinsonism.

11
E t i o l o g y According the modern investigations in base of this disease is inborn dificiency of tyrosintransferase enzyme in dopamine. Parkinsonism may be defined in biochemical term as an inborn dopamine deficiency state.

12
Basic symptoms of Parkinsons syndrome: Hypokinesia (Akinesia) Rigidity Tremor
 Rigidity Tremor")
13
The main pathogenetic mechanisms: Great cell loss in the substantia nigra, low concentration of dopamine in striatum, the influence of striatum on pallidum. As a result akinesia occurs. The main cause of rigidity is increasing of tonic reflex on muscles tension. The main source of tremor is thalamus ( its nucleus ventrolateralis ).

14
Hypokinesia (Akinesia) Bradykinetic and akinetic state The gait is shuffling and the steps are slight Parallel footprints The loss of associated swinging of the arm or arms when walking - (acheirokynesis) A lack of mobility of facial expression (Bechterevs symptome) Infrequent blinking of the eyelids (Mary s symptome) Fixed look
 Bradykinetic and akinetic state The gait is shuffling and the steps are slight Parallel footprints The loss of associated swinging of the arm or arms when walking - (acheirokynesis) A lack of mobility of facial expression (Bech")
15
Hypokinesia (Akinesia) Inertia of rest (that means it is very difficult for patient to start moving) Inertia of movement (the so-called propulsive gait, lateropusion or retropulsion) Micrography – handwriting is too small Speach is quite and inexpressive (bradylalia) Paradoxical kynesia is possible after strong impression or great emotions
 Inertia of rest (that means it is very difficult for patient to start moving) Inertia of movement (the so-called propulsive gait, lateropusion or retropulsion) Micrography – handwriting is too small Speach is quite and inexpres")
16
Rigidity plastic type of increased muscle tone: Cogged-wheel symptom (in carporadial joint) Tonus increases in course of evaluation of nervous system state Tonus is expressed in the same manner in the group of flexors and extensors
 Tonus increases in course of evaluation of nervous system state Tonus is expressed in the same manner in the group of flexors and extensors")
17
Tremor: Are much more expressed in distal parts of extremities, sometimes tremor of lips or lower jaw can occur It looks like coins counting It is much more expressed while resting. It disappears or decreases while moving Its frequency is 3 – 6 times per second

18
Other features of Parkinsons disease Bradyphrenia (thoughts are too slow) Bradymnesia (recollection is slow too) While speaking such patients are boring (akairia - Astwatsaturov symptome) Usually they are in a bad mood. Depression is very typical for the patients with Parkinson disease Sometimes they have autonomic disorders Parasympathetic nervous system dominates in such patients – they have running saliva (aeriel symptome), hyperhydrosis, fatty skin and type of hair, bradicardia and arterial hypotension
 Bradymnesia (recollection is slow too) While speaking such patients are boring (akairia - Astwatsaturov symptome) Usually they are in a bad mood. Depression is very typical for")
19
T e s t s: The symptom of air pillow or Vartenberg symptom – The patient is lying down. One props up his head a little bit and then quickly takes his hand out. Normally the head is falling down. But in patients with Parkinson disease the head stays in the same position for a while.

20
T e s t s: Westfahls phenomena of paradoxical muscle constriction – While foot extension it stays in the same position for a while. Hand extension test. Test of knee flexion – The patient is lying on his abdomen; his lower extremities are bended in knees. In patients with Parkinson disease the legs are fixed in this position for several minutes.

21
Tests: The symptom of Noica–Haneva While evaluations of muscle tone one asks the patient to raise his opposite extremity. In patients with Parkinson disease the tonus suddenly increases.

22
Clinical forms of Parkinson disease: Rigid (hypokynesia dominates) Trembling Mixed : rigid – trembling or trembling – rigid
 Trembling Mixed : rigid – trembling or trembling – rigid")
23
The degree of severity (according to Petelin): The first degree - expressed one or two main symptoms. The patient preserves professional and home activity The second degree – The patient is disabled professionally The third degree – The patient cannot take care of himself
: The first degree - expressed one or two main symptoms. The patient preserves professional and home activity The second degree – The patient is disabled professionally The third degree – The patient canno")
24
Symptomatic Parkinsonism Craniocerebral trauma ( Muhammad Ally) CO, Mn intoxication Brain tumor Encephalitis (Economo) Strokes Cerebral atherosclerosis Medicinal parkinsonism (reserpinum, neuroleptics) Poisoning of heavy metals
 CO, Mn intoxication Brain tumor Encephalitis (Economo) Strokes Cerebral atherosclerosis Medicinal parkinsonism (reserpinum, neuroleptics) Poisoning of heavy metals")
27
Hyperkynetic–hypotonic syndrome: The main clinical signs of this syndrome are: Muscular hypotonia Involuntary movements – hyperkynesis. Involuntary movements are characterized by: the amplitude of the movement location of muscle involved the rate the duration of contraction and the relaxation

28
Kinds of hyperkynesis Chorea Athetosis Choreoathetosis Ballism and hemiballism Myoclonus Torsion spasm Tics Facial cramp Tremor

29
C h o r e a spontaneous, irregular, purposeless and asymmetric movements they are present at rest and subside during sleep eyes and tongue symptom ( or Hersonskys symptom ) - the patients are unable to maintain tongue protrusion for more than a few seconds; Hordons II symptom – while checking knee – reflex crus stays in the position of extension for a while and then slowly goes down; Cherni symptom - pathologic sudden abdomen at breath. The most common diseases - Huntingtons chorea (inherited disease), rheumatic subcortical encephalitis or chorea Sydenhams (juvenile disease), atherosclerotic chorea, chorea gravidarum, electric chorea.
 - the patients are unable to maintain tongue protrusion for more than a few s")
30
A t h e t o s i s Movements are slower and more sustained than choreiform movements they affect primarily the distal portion of extremities snakelike movement of any combination of flexion, extension, adduction and abduction in varying degrees They are regularly associated with increased muscular tone It is supposed that athetosis is the result of nucleus caudated lesion. Choreoathetosis is a term selected to describe movements that are intermediate between chorea and athetosis.

31
Ballism and hemiballism Its the more or less continues gross abrupt contractions of axial and proximal muscles of the extremities In the most cases this movement disorder is confined to one side of the body (hemiballism) It may be associated with hypotonia
 It may be associated with hyp")
32
Torsion spasm Twisting or turning movements The muscles of trunk and neck are involved Sometimes torticollis can occur Usually it is the result of putamen lesion

33
Myoclonus Is a jerking movement of one or more muscle groups (for example palatine, tongue, pharynx, larynx, diaphragm and skeletal muscles) Usually only one muscle group is involved They are synchronous in most of cases and sometimes they are asynchronous Their frequency is about 15 – 18 per minute They may be induced by visual, tactile, or auditory stimuli (stimulus-sensitive myoclonus) or by the initiation of the voluntary movement (intention myoclonus).
 Usually only one muscle group is involved They are synchronous in most of cases and sometimes they are asynch")
34
T i c s are an involuntary compulsive stereotyped movements they may be simple or complex tics may involve any portion of the body ( they are most common about the face where they are manifest as blinking, grinning, smirking, lip licking, nose wrinkling) Facial cramp is tonic seizure in facial muscles Tremor Is rhythmical jerking of arms, legs or head Its frequency is about 4 – 6 per second

38
C e r e b e l l u m is a reflexional organ of coordination of movements, equilibrium and muscular tone

39
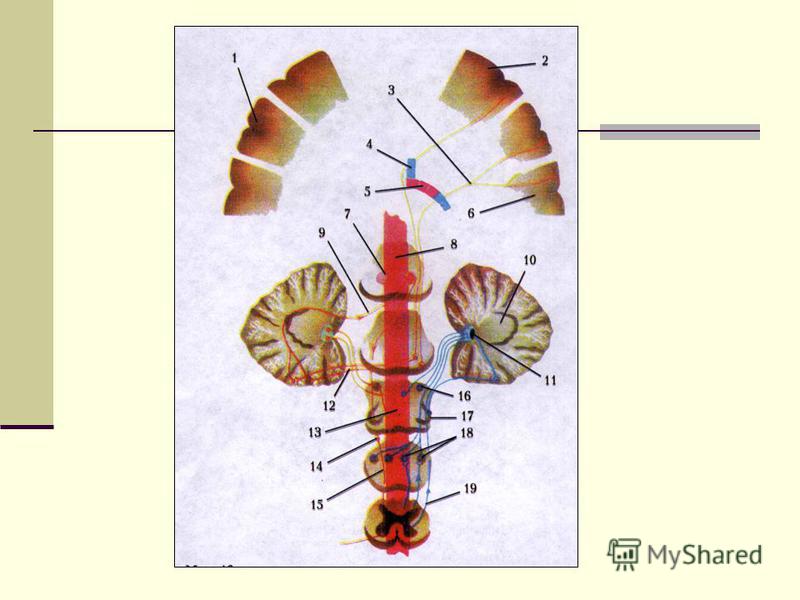
C e r e b e l l u m Contains : Two large lateral hemispheres Flocculo-nodular lobe (vermix) Three pairs of peduncles.
 Three pairs of peduncles.")
40
Grey matter of cerebellum Is presented by cortex of hemispheres and nuclei of cerebellum: Nucleus fastigii Nucleus globosus Nucleus emboliformis Nucleus dentatus

41
Cerebellum peduncles: The lower peduncles (corpora restiformia) provide connection with oblong brain and spinal cord: Tr. spinocerebellaris dorsalis (Flexigs) Tr. vestibulocohlearis (from nuclei vestibularis to nucleus fastigii) Tr. olivocerebelaris (from lower olives to nucleus dentatus) Fibre arcuate externe (from nuclei Holl and Burdach to hemispheres and vermis)
 provide connection with oblong brain and spinal cord: Tr. spinocerebellaris dorsalis (Flexigs) Tr. vestibulocohlearis (from nuclei vestibularis to nucleus fastigii) Tr. olivocerebelaris")
42
Cerebellum peduncles: The middle peduncles (pedunculum cerebellaris medii) provide connection with pons Tr. pontocerebellaris. They connect nuclei of pons with the opposite hemisphere of cerebellum
 provide connection with pons Tr. pontocerebellaris. They connect nuclei of pons with the opposite hemisphere of cerebellum")
43
Cerebellum peduncles: The upper peduncles of cerebellum (pedunculi cerebellaris superior) connect cerebellum with middle brain. They include two systems: Afferent one – from spinal cord to cerebellum – tr. spinocerebellaris ventralis (Hovers) Efferent one – from cerebellum to the structures of extrapyramidal nervous system – tr. cerebellotegmentalis et tr. dentorubralis.
 connect cerebellum with middle brain. They include two systems: Afferent one – from spinal cord to cerebellum – tr. spinocerebellaris ventralis (Hovers) Efferen")
44
The way of cerebellum correction The first neuron – tr. fronto-temporo – occipito- pontinus The second neuron – tr. pontocerebellaris (pontino- cerebellaris decussation) The third neuron – tr. cerebello – dentatus The forth neuron – tr. dentorubralis (Vernekinks decussation) The fifth neuron – tr. rubrospinalis (Forels decussation) The sixth neuron – tr. spinomuscularis
 The third neuron – tr. cerebello – dentatus The forth neuron – tr. dentorubralis")
46
The main functions of cerebellum: body equilibrium regulation of muscle tone coordination of movements synergy

47
Vermix function are: Equilibrium of the body Regulation of muscle tone Hemispheres function are: Coordination of the movements of extremities Synergy of the muscle

48
A t a x i a means disturbances of equilibrium of the body and coordination of movements. Cerebellum lesion produces cerebellar ataxia: Static (lesion of vermix) Dynamic (lesion of hemispheres)
 Dynamic (lesion of hemispheres)")
49
Kinds of ataxias: Cerebellar ( cerebellum lesion ) Sensitive ( loss of deep joint sense ) Frontal (cortical) ( lesion of Frontal lobe ) Vestibular ( lesion of vestibular apparatus ) Hysterical ( in case of Hysteria ) Mixed
 Sensitive ( loss of deep joint sense ) Frontal (cortical) ( lesion of Frontal lobe ) Vestibular ( lesion of vestibular apparatus ) Hysterical ( in case of Hysteria ) Mixed")
50
Cerebellar ataxia Attactic gait – patient cant to walk Disorders of equlibrium – patient cant to stand Muscular hypotonia Intention tremor – is dynamic tremor (it is more expressed while moving and disappears while rest) Nystagmus: horizontal, vertical, vertical rotary, or dissociated (different in each eye) Scanning speech –patient cant to speak slowly Macrographia – handwriting is too large Dysmetria (disturbed ability to gauge distances) Adiadochokinesia (disturbed ability to perform rapid alternating movements) Asynergia – disturbed ability to controls function of antagonists muscles
 Nystagmus: horizontal, vertic")
51
Symptoms of lesion Cerebellar lower peduncles lesion can cause: Cerebellar ataxia Bulbar syndrome Sometimes pathology of Holls and Burdachs nuclei is associated with this lesion. Then ataxia is complex and is called cerebellar – sensitive ataxia. Cerebellar upper peduncles lesion can cause: Cerebellar ataxia at the side of lesion Trochlear Nerve lesion Midbrain lesion symptoms

52
Symptoms of lesion Nucleus ruber lesion can cause: Cerebellar ataxia in the opposite extremities Resting tremor Webbers syndrome or paresis of convergence may occur Pontino – cerebellar angle lesion manifests as: Cerebellar disorders and pathology of VII, VIII, V, VI pairs of CNs at the side of lesion Pyramidal and sensory hemisyndrome on the opposite side

Еще похожие презентации в нашем архиве:





 – is a part of clinical medicine, which is involved in.")








, I (for infectious) and R (for recovered). Therefore, this.")

 по теме: презентация по английскому языку Ecological problems")







 real-life sources of data, the leading.")