Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Gallbladder Cancer

3
Epidemiology Incidence ~ th most common GI malignancy Women > men High incidence in S America (Chile) ~ 1% of pts undergoing cholecystectomy for symptomatic gallstones
 ~ 1% of pts undergoing cholecystectomy for symptomatic gallstones")
4
Risk Factors Gallstones Gallbladder Polyps Chronic Salmonella infection Abnormal Pancreaticobiliary duct junction * Porcelain gallbladder * Age

5
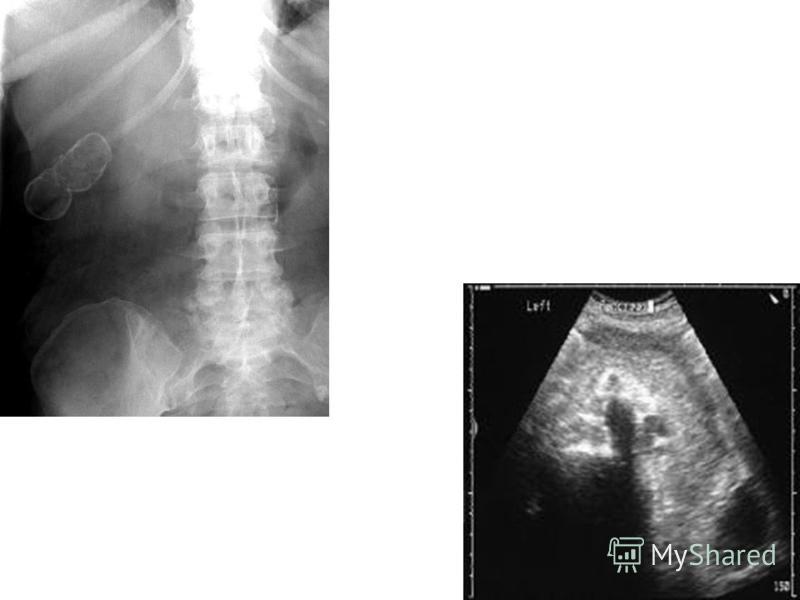
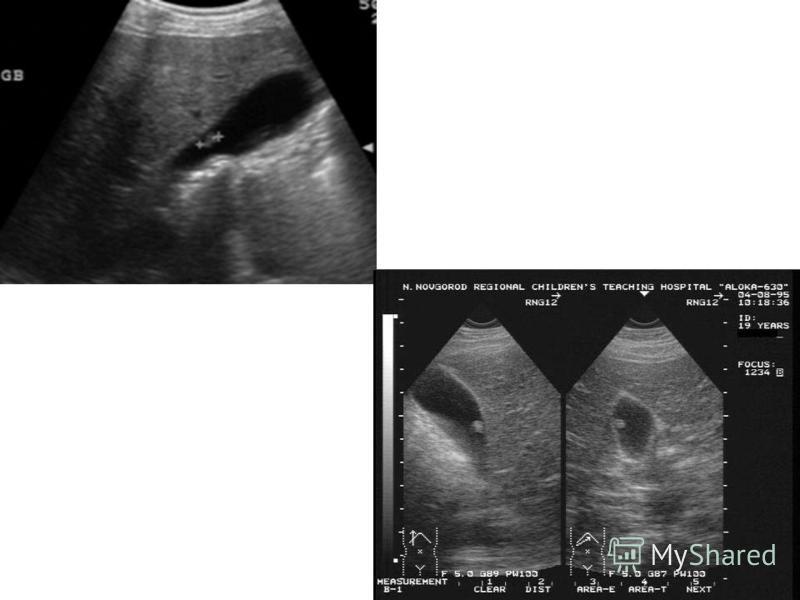
Presentation/Diagnostic Imaging Presentation is non-specific Diagnositic Imaging –Sono –CT –MR/MRCP –EUS

9
Histology / Pathology * Progression to Ca may take up to 15 yrs Adenocarcinoma 80-90% Anaplastic 7% Squamus 6% Lymphoma, Sarcoma

10
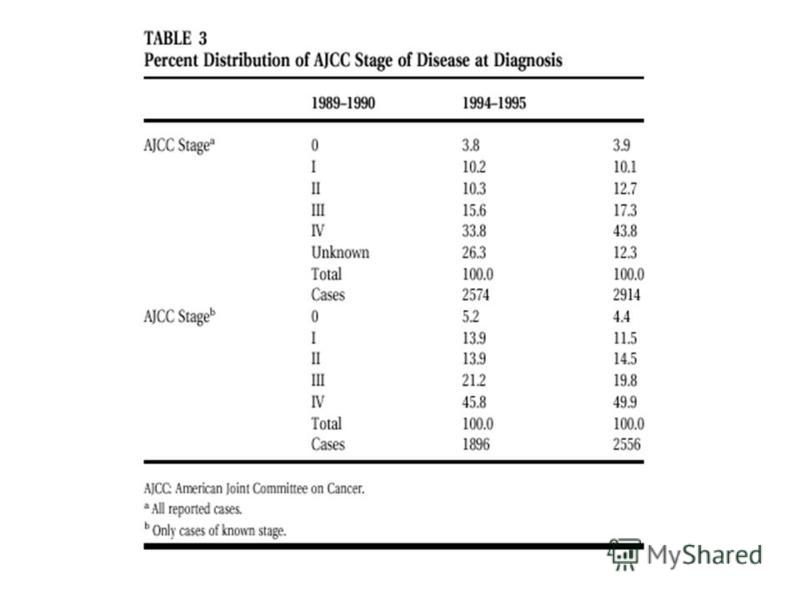
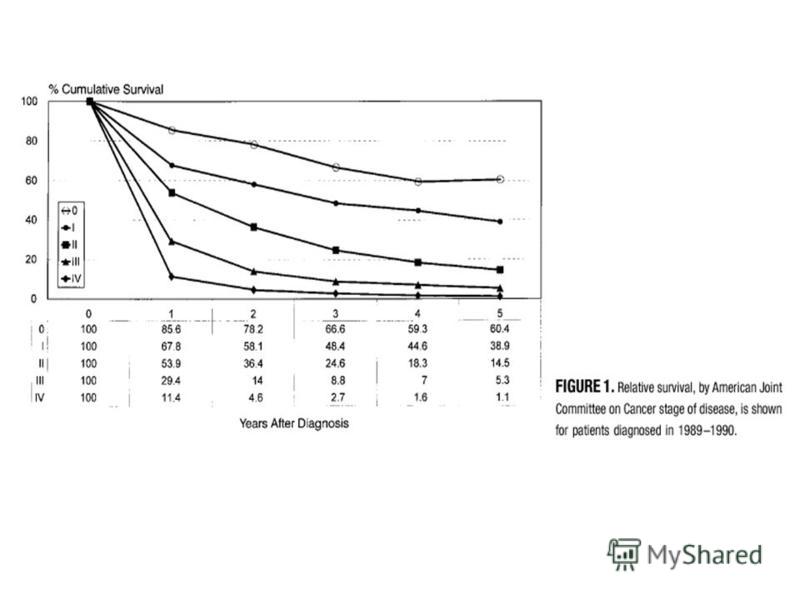
Staging

13
Surgical Management Only 10-30% time of diagnosis Three Presentations: –GB CA discovered during or after lap/open chole for assumed benign dz –GB CA suspected after diagnostic evaluation –GB CA advanced stage at presentation

14
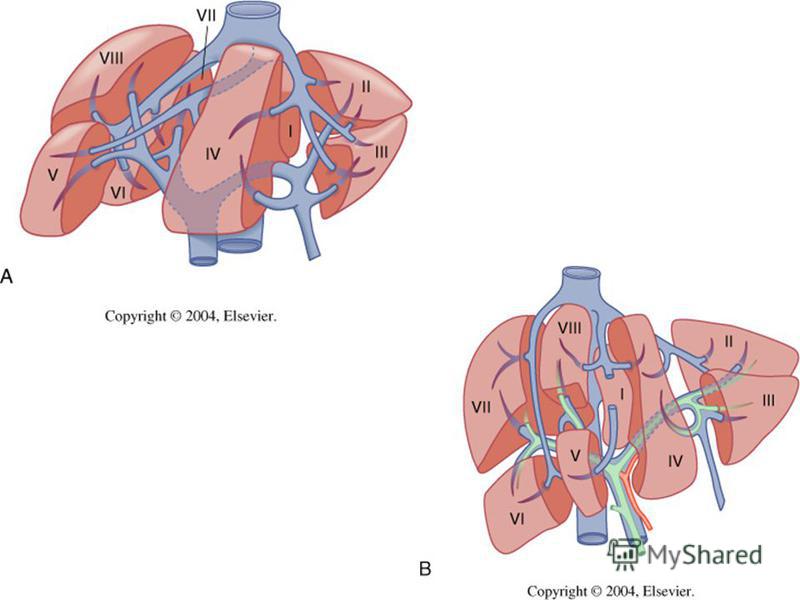
Surgical Options Simple cholecystectomy Radical cholecystectomy Radical chole w/ anatomic liver resection Radical chole w/ Whipple

17
What to do during elective lap chole if GB Ca is suspected intraoperatively ? ~ 0.5 % of asx cases found to have GB CA in lap chole Convert to OPEN Resect PORTS No place for laparoscopic resection

18
Management of T1 lesions 5Yr survival rates have improved for T1a dz following simple cholecystectomy % T1b (muscularis) is controversial –Simple v radical chole –Wakai (2001) – 10 yr survival for T1b tumors after simple chole was 87%
 is controversial –Simple v radical chole –Wakai (2001) – 10 yr survival for T1b tumors after simple chole was 87%")
19
Management of T2 lesions Incidentally detected GB Ca in specimen Re-exploration w/ radical chole for T2 lesions or greater MSKCC (1998) – improved disease free survival from ~ 20 60% –De Aretxabala Chile (1997) showed improvement from 20% 70% 5Yr survival
 – improved disease free survival from ~ 20 60% –De Aretxabala Chile (1997) showed improvement from 20% 70%")
20
Management of locally advanced T3/T4 lesions High morbidity & mortality rates (~50% & 15%) Reluctance to operate because of poor prognosis Nakamura (1999) found extensive surgery for stage IV pts showed significant improvement in 5Yr survival when compared to palliative operation/unresectable dz
 Reluctance to operate because of poor prognosis Nakamura (1999) found extensive surgery for stage IV pts showed significant improvement in 5Yr survival when co")
21
Management of locally unresectable dz (major vascular encasement) NO DEBULKING Chemoradiotherapy –No identified impact on survival & remains investigational –Systemic chemotherapy – no optimal regimen defined (5-FU based)
 NO DEBULKING Chemoradiotherapy –No identified impact on survival & remains investigational –Systemic chemotherapy – no optimal regimen defined (5-FU based)")
22
Contraindications to resection Mets to liver, peritoneum, or encasement of major vessels Direct involvement of adjacent organs is NOT absolute contraindication

Еще похожие презентации в нашем архиве:




 A neurosurgeon is a surgeon who specializes in operating on the brain, head, neck, and spinal cord.")
 Professor of Neurosurgery Northwestern University Feinberg School of Medicine.")









 (GP2 Year 2010) LG Electronics/ LCD TV Division Feb. 17 th, 2010 - Applied Models & Notice - File Copy - User Download Mode.")




 Ventilator-associated pneumonia (VAP) is defined as nosocomial pneumonia in a patient on mechanical ventilatory support.")