Скачать презентацию
Идет загрузка презентации. Пожалуйста, подождите

1
Obstetrics/Gynecology Emergency Medical Technician - Basic

2
Female Reproductive System Uterus Cervix Vagina Urinary Bladder Rectum

3
Female Reproductive System Uterus Vagina Fallopian tube Ovary Cervix

4
OB/Gyn Assessment zHistory yWhen was your last normal menstrual period (LNMP)? yAbdominal pain? (location/quality) yVaginal bleeding/discharge?
? yAbdominal pain? (location/quality) yVaginal bleeding/discharge?")
5
OB/Gyn Assessment zHistory yIs there a possibility you might be pregnant? xMissed period? xN/V xIncreased urinary frequency xBreast enlargement xVaginal discharge

6
OB/Gyn Assessment zHistory yIf pregnant: xPara = # of live births xGravida = # of pregnancies x-3 /+ 7 to estimate due date Subtract 3 from the month of the LNMP Add 7 to the date of the LNMP LNMP - 12/9/98 Due date - 9/16/99

7
OB/Gyn Assessment zVital signs yHypertension yHypotension yTilt test if blood loss is suspected zFocused exam yEdema (particularly of face, hands)
")
8
Gyn Emergencies

9
Ectopic Pregnancy z Zygote implants in location other than uterine cavity z 95% are in Fallopian tube (tubal ectopic) z Life threatening!
 z Life threatening!")
10
Ectopic Pregnancy zSigns and Symptoms yMissed period, other signs/symptoms of early pregnancy yLight vaginal bleed (spotting) 6-8 weeks after LNMP yAbdominal pain, may radiate to shoulder yPositive tilt test yOther signs/symptoms of hypovolemic shock
 6-8 weeks after LNMP yAbdominal pain, may radiate to shoulder yPositive tilt test yOther signs/symptoms of hypovolemic shock")
11
Ectopic Pregnancy zSigns and Symptoms yAbdominal pain may be absent ySome patients may NOT miss period ySome patients may have NEGATIVE pregnancy tests

12
Ectopic Pregnancy Lower abdominal pain or unexplained hypovolemic shock in a woman of child-bearing age equals Ectopic Pregnancy Until Proven Otherwise

13
Ectopic Pregnancy zManagement y100% O 2 ySupportive care for hypovolemic shock yTransport immediately

14
Pelvic Inflammatory Disease zAcute or chronic infection zInvolves Fallopian tubes, ovaries, uterus, peritoneum zMost commonly caused by gonorrhea zStaph, strep, coliform bacteria also cause infections

15
Pelvic Inflammatory Disease zSigns and Symptoms yLower abdominal pain yGradual onset over 2-3 days, beginning 1-2 weeks after last period yFever, chills yNausea, vomiting yYellow-green vaginal discharge yWalks bent forward, holding abdomen

16
Pelvic Inflammatory Disease zManagement yHigh concentration O 2 yTransport

17
Spontaneous Abortion zMiscarriage zPregnancy terminates before 20th week zUsually occurs in first trimester (first three months)
")
18
Spontaneous Abortion zSigns and Symptoms yVaginal bleeding yCramping lower abdominal pain or pain in back yPassage of fetal tissue

19
Spontaneous Abortion zComplications yIncomplete abortion yHypovolemia yInfection, leading to sepsis

20
Spontaneous Abortion zManagement yHigh concentration O 2 yShock position yTransport any tissue to hospital yProvide emotional support

21
Pre-eclampsia zAcute hypertension after 24th week of gestation z5-7% of pregnancies zMost often in first pregnancies zOther risk factors include young mothers, no prenatal care, multiple gestation, lower socioeconomic status

22
Pre-eclampsia zTriad yHypertension yProteinuria yEdema

23
Pre-eclampsia zSign and Symptoms yHypertension xSystolic > 140 mm Hg xDiastolic > 90mm Hg xOr either reading > 30 mmHg above patients normal BP yEdema (particularly of hands, face) present early in day
 present early in day")
24
Pre-eclampsia zSigns and Symptoms yRapid weight gain x>3lbs/wk in 2nd trimester x>1lb/wk in 3rd trimester yDecreased urine output yHeadache, blurred vision yNausea, vomiting yEpigastric pain yPulmonary edema

25
Pre-eclampsia zComplications yEclampsia yPremature separation of placenta yCerebral hemorrhage yRetinal damage yPulmonary edema yLower birth weight infants

26
Pre-eclampsia zManagement y100% O 2 yLeft lateral recumbent position yAvoid excessive stimulation yReduce light in patient compartment yAvoid use of emergency lights, sirens

27
Eclampsia zGravest form of pregnancy-induced hypertension zOccurs in less than 1% of pregnancies

28
Eclampsia zSigns and Symptoms ySigns, symptoms of pre-eclampsia plus: xGrand mal seizures xComa

29
Eclampsia zComplications ySame as pre-eclampsia yMaternal mortality rate: 10% yFetal mortality rate: 25%

30
Eclampsia zManagement y100% O 2 ; assist ventilations, as needed yLeft lateral recumbent position yReduce light yManage like any major motor seizure yEmergency transport yConsider ALS intercept for anticonvulsant medication administration

31
Eclampsia zAssess every pregnant patient for yIncreased BP yEdema zTake all reports of seizures in pregnant females seriously

32
Abruptio Placentae zPremature separation of placenta from uterus zHigh risk groups yOlder pregnant patients yHypertensives yMultigravidas

33
Abruptio Placentae zSigns and Symptoms yMild to moderate vaginal bleeding yContinuous, knife-like abdominal pain yRigid, tender uterus ySigns, symptoms of hypovolemia

34
Abruptio Placentae Third Trimester Abdominal Pain equals Abruptio Placentae until proven otherwise

35
Abruptio Placentae Hypovolemic shock out of proportion to visible bleeding equals Abruptio Placentae until proven otherwise

36
Abruptio Placentae zManagement y100% O 2 yLeft lateral recumbent position ySupportive care for hypovolemic shock yRapid transport

37
Placenta Previa zImplantation of placenta over cervical opening

38
Placenta Previa zSigns and Symptoms yPainless, bright-red vaginal bleeding ySoft, non-tender uterus ySigns and symptoms of hypovolemia

39
Placenta Previa zManagement y100% O 2 yLeft lateral recumbent position ySupportive care for hypovolemic shock yNever perform a vaginal exam on a pt in the 3rd trimester with vaginal bleeding

40
Placenta Previa A vaginal exam should NEVER be performed on a patient in the 3rd trimester with vaginal bleeding

41
Uterine Rupture zCauses yBlunt trauma to pregnant uterus yProlonged labor against an obstruction yLabor against weakened uterine wall xOld Cesarian section scar xGrand multiparous patients

42
Uterine Rupture zSigns and Symptoms yTearing abdominal pain ySevere hypovolemic shock yFirm, rigid abdomen yPossible palpation of fetal parts through abdominal wall yVaginal bleeding may or may not be present

43
Uterine Rupture zManagement y100% O 2 yAnticipate shock yALS/helicopter intercept

44
Emergency Childbirth

45
Developing Fetus Placenta Amniotic Sac Bag of waters Umbilical cord Fetus

46
Labor z1st stage: Onset of contractions to dilation of cervix z2nd stage: Complete dilation of cervix to delivery of baby z3rd stage: Delivery of baby to delivery of placenta

47
Signs of Imminent Delivery zCrowning zRupture of Amniotic Sac zNeed to bear down zSensation of needing to move bowels zContractions y1 to 2 minutes apart yRegular yLasting 45 to 60 seconds

48
Delivery zPlace gloved hand on presenting part to prevent explosive delivery zOn delivery of head, suction mouth then nose

49
Delivery zGently guide babys head down to deliver upper shoulder zGently guide babys head up to deliver lower shoulder zGently assist with delivery of rest of baby; Do NOT pull zNote time of delivery of baby

50
Delivery zControl slippery baby during delivery ySupport head, shoulders, feet yKeep head lower then feet to facilitate drainage of secretions from mouth zDry baby zKeep baby warm

51
Delivery zClamp, cut cord yFirst clamp about 4 from baby ySecond clamp 2 further away from first yCut between clamps yUse umbilical tape to control any bleeding from cord

52
Delivery zFlick babys feet, rub back to stimulate zDo NOT shake infant zDo NOT slap buttocks zBlow by O 2 if: yHeart rate < 100 yPersistent central cyanosis present zResuscitate if necessary

53
Delivery zDeliver Placenta yPlace placenta in plastic bag and deliver to hospital to be examined for completeness yIf placenta does not deliver within 10 minutes, transport

54
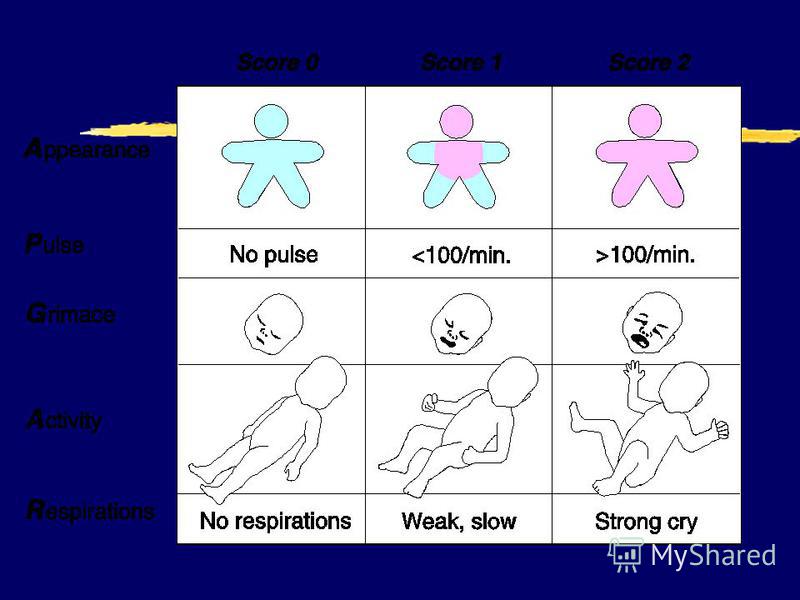
APGAR Score zDeveloped by Virginia Apgar zQuick evaluation of infants pulmonary, cardiovascular, neurological function zUseful in identifying infants needing resuscitation

56
APGAR Score Determine at 1 and 5 minutes postpartum!

57
Maternal Care: Postpartum zBleeding yPlace sterile pad over vaginal opening yIf bleeding is excessive: xRapidly transport to hospital xUterine massage xEncourage breastfeeding

58
Maternal Care: Postpartum zShock yIf mother shows signs, symptoms of shock: xHigh concentration O 2 xRapid transport xALS intercept

59
Complicated Deliveries

60
Breech Presentation

61
zManagement yHigh concentration O 2 yRapid transport yPrepare for neonatal resuscitation yAssist delivery

62
Breech Presentation zManagement yIf head does not deliver within 3 minutes of body: xInsert gloved hand into vagina forming V around babys nose, mouth xPush vaginal wall away from babys face to create airway

63
Limb Presentation

64
zManagement yHigh concentration O 2 yRapid transport

65
Prolapsed Cord zUmbilical cord enters vagina before infants head zPressure of head on cord occludes blood flow, O 2 delivery to fetus

66
Prolapsed Cord zManagement yHigh concentration O 2 yKnee-chest position or exaggerated shock position yPlace gloved hand in vagina yApply gentle pressure inward to presenting part; relieve pressure on cord

67
Umbilical Cord around Neck zManagement yUpon delivery of head look for cord is looped around neck yGENTLY slip cord over head if possible yIf cord cannot be slipped over head: xClamp in two places xCut between clamps with surgical scissors

68
Amniotic Sac Intact zManagement yUse clamp to tear sac, release fluid yMove sac away from babys nose, mouth

69
Meconium zFirst stool of newborn zMeconium-stained amniotic fluid yBaby has had bowel movement in utero yGreenish, black (pea soup) color yIndicative of distress
 color yIndicative of distress")
70
Meconium zMeconium can: yOcclude airway yCause pneumonitis

71
Meconium zManagement yAvoid early stimulation of baby to prevent aspiration yAggressively suction airway until all meconium is removed

72
Multiple Births

73
zConsider as possibility if: yMothers abdomen appears abnormally large prior to delivery yMothers abdomen remains large after delivery of first baby yContractions continue after delivery of first baby

74
Multiple Births zDelivery yClamp cord of first baby before delivery of second yUsually second baby will deliver shortly after first yCare for babies, mother, and placenta(s) as you would in a single birth
 as you would in a single birth")
75
Multiple Births zMultiple babies are usually small zIt is important to keep them warm!

76
Premature Infants zDefinition y< 28 weeks gestation, or y< 5.5 pounds birth weight

77
Premature Infants zManagement yKeep baby warm yKeep airway clear yAssist ventilations if necessary yResuscitate if necessary yWatch umbilical cord for bleeding yBlow by O 2 yAvoid contamination yConsider ALS intercept

Еще похожие презентации в нашем архиве:













, I (for infectious) and R (for recovered). Therefore, this.")